Important: This page is for informational purposes only, based on published peer-reviewed research and official UK dietary guidelines (NHS, EFSA, SACN). It does not constitute medical advice. Always consult your GP or pharmacist before starting, stopping, or combining supplements.
Supplements Studied for General Wellness
A foundational stack covering the most common nutritional gaps in the UK
Why This Stack?
Four nutrients consistently emerge from UK dietary surveillance data as the most under-consumed by adults: vitamin D, magnesium, omega-3 fatty acids, and vitamin K2. Addressing these gaps forms the basis of a general wellness stack grounded in population-level evidence rather than trend-driven marketing. The logic is straightforward: before reaching for exotic botanicals or niche compounds, it makes sense to correct the foundational shortfalls that affect millions of people across the country. The National Diet and Nutrition Survey (NDNS) rolling programme — most recently reporting on fieldwork from 2019 to 2023, published in June 2025 — found that 18% of UK adults aged 19 to 64 were vitamin D deficient, rising to 31% during winter months when UVB exposure is minimal. SACN's 2016 vitamin D report recommended a Reference Nutrient Intake of 10 micrograms (400 IU) daily for everyone aged four and above throughout the year, yet only 17% of working-age adults reported taking a vitamin D supplement. Magnesium intake tells a parallel story: NDNS data show that a meaningful proportion of UK adults — particularly younger women and men with irregular eating patterns — fall below the Lower Reference Nutrient Intake, the threshold below which deficiency is likely. Oily fish consumption, the primary dietary source of long-chain omega-3 fatty acids, remains well below recommended levels across all age groups in the NDNS rolling programme data. For younger adults and women of childbearing age, the shortfall is particularly pronounced. Vitamin K2 lacks a formal UK RNI, but its role in calcium metabolism — directing calcium toward bone tissue and away from soft tissues such as arterial walls — makes it a logical companion to vitamin D3 supplementation. Without K2, increasing calcium absorption through vitamin D supplementation may not translate into the bone and cardiovascular benefits that most people are seeking. Together, these four ingredients target the nutritional shortfalls that affect the broadest cross-section of the UK adult population, using doses that sit within established safety margins and do not require medical supervision for otherwise healthy individuals. This is not a stack designed to optimise athletic performance or treat a specific condition. It is a baseline intended to fill the gaps that diet and limited sunlight exposure leave behind.
What’s in This Stack
Vitamin D3
2,000 IUSACN recommends 10mcg/day for all UK adults. PHE data shows 1 in 5 adults are deficient, rising to 1 in 3 in winter. The single most impactful supplement for the average UK resident.
Available Forms
| Form | Bioavailability | Notes |
|---|---|---|
| Cholecalciferol (D3) | high | Preferred form; raises serum 25(OH)D more effectively than D2 |
| Ergocalciferol (D2) | moderate | Vegan-friendly (plant/fungal) but less potent per IU |

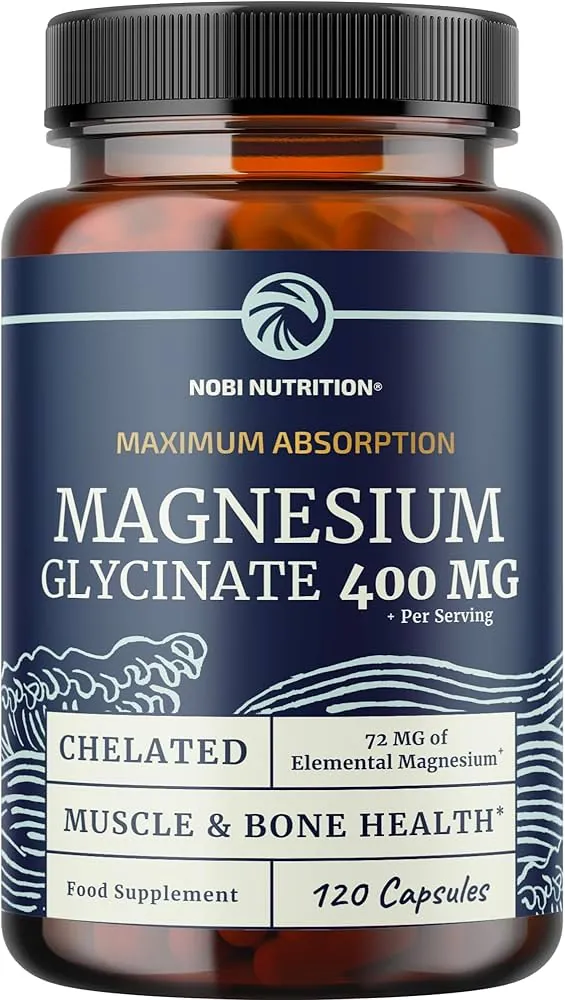
Magnesium
300–400mg (glycinate or citrate)National Diet and Nutrition Survey data suggests many UK adults fall short of the 300mg/day RNI. Magnesium supports sleep, muscle function, and over 300 enzymatic processes.
Available Forms
| Form | Bioavailability | Notes |
|---|---|---|
| Magnesium Glycinate | high | Chelated form, well-absorbed, least likely to cause GI issues, calming effect |
| Magnesium Citrate | high | Good absorption, mild laxative effect at higher doses |
| Magnesium Oxide | low | ~4% bioavailability, primarily used as laxative, poor supplement choice |
| Magnesium Taurate | high | Combined with taurine, studied for cardiovascular and sleep support |
| Magnesium L-Threonate | high | Crosses blood-brain barrier, studied for cognitive function |


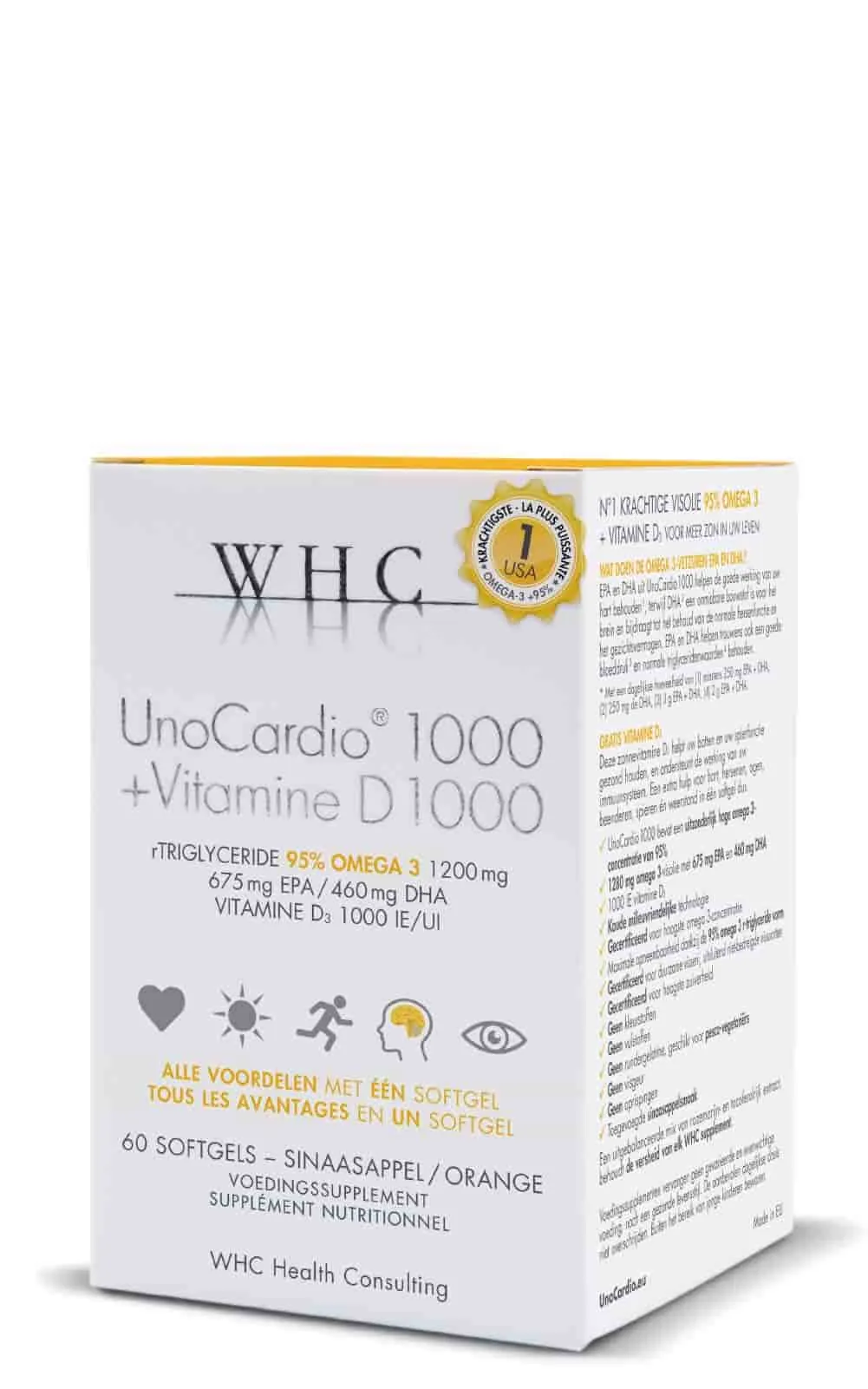
Omega-3
1,000–2,000mg EPA+DHAThe UK population eats significantly less oily fish than recommended. Omega-3 supports cardiovascular health, brain function, and may reduce systemic inflammation (NICE guidelines).
Available Forms
| Form | Bioavailability | Notes |
|---|---|---|
| Triglyceride (rTG) Fish Oil | high | Re-esterified triglyceride, best absorbed form, premium |
| Ethyl Ester (EE) Fish Oil | moderate | Most common, requires more processing by the body, cheaper |
| Algae Oil (DHA-rich) | high | Vegan source, primarily DHA, sustainable |
| Krill Oil | high | Phospholipid-bound, contains astaxanthin, well-absorbed but lower EPA+DHA per capsule |


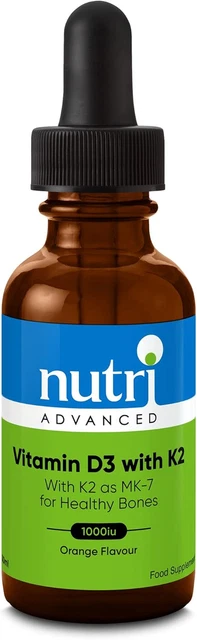
Vitamin K2
100mcg (MK-7)Research suggests K2 works synergistically with Vitamin D3 to direct calcium to bones and away from soft tissues. Most Western diets are low in K2 (Vermeer, 2012, Blood).
Available Forms
| Form | Bioavailability | Notes |
|---|---|---|
| MK-7 (Menaquinone-7) | high | Longer half-life (~72h), most studied form for bone and cardiovascular health |
| MK-4 (Menaquinone-4) | moderate | Shorter half-life (~4h), requires higher doses |

How This Stack Works
Each ingredient in this stack addresses a distinct physiological system, and the evidence supporting their inclusion draws on both mechanistic research and population-level dietary data.
Vitamin D3 operates as a secosteroid hormone precursor rather than a simple micronutrient. Once hydroxylated in the liver and kidneys to its active form (1,25-dihydroxyvitamin D), it binds to vitamin D receptors expressed across a wide range of tissues. In bone, it facilitates intestinal calcium absorption — without adequate vitamin D, the body absorbs only 10 to 15% of dietary calcium compared to 30 to 40% under sufficient conditions. Aranow (2011, Journal of Investigative Medicine) reviewed the immunological role of vitamin D and noted that the vitamin D receptor is expressed on B cells, T cells, and antigen-presenting cells, with deficiency associated with increased susceptibility to infection. SACN's 2016 report established the 10 microgram daily RNI to maintain serum 25(OH)D above the 25 nmol/L threshold linked to musculoskeletal risk. However, many researchers and clinicians consider 50 nmol/L a more appropriate target for broader health outcomes. A daily dose of 2,000 IU (50 micrograms) remains well within the NHS-stated upper limit of 4,000 IU and is a common choice for individuals seeking to reach and maintain sufficient serum levels, particularly between October and March.
Magnesium functions as a cofactor in over 300 enzymatic reactions, including those governing ATP production, DNA and RNA synthesis, and neuromuscular function. Its relevance to general wellness extends across energy metabolism, nervous system regulation, and blood pressure homeostasis. NDNS data consistently show that a meaningful proportion of the UK adult population fails to meet adequate intake levels from diet alone, with women aged 65 and over showing a gradual worsening trend over the survey period. The forms recommended here — glycinate and citrate — are organic magnesium salts with higher bioavailability and better gastrointestinal tolerability than magnesium oxide. EFSA set a supplemental tolerable upper intake level of 250mg from readily dissociable magnesium salts (separate from dietary intake) based on the threshold below which osmotic diarrhoea is unlikely, while the UK Expert Group on Vitamins and Minerals (EVM) set a higher guidance level of 400mg supplemental. A starting dose of 200 to 300mg supplemental elemental magnesium is prudent, increasing gradually if tolerated. Chelated forms such as glycinate and citrate tend to cause less gastrointestinal discomfort than magnesium oxide, partly because they are absorbed more efficiently and exert a weaker osmotic effect in the gut.
Omega-3 fatty acids — specifically EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) — serve as structural components of cell membranes and precursors to specialised pro-resolving mediators that modulate inflammatory responses. Khan et al. (2021, eClinicalMedicine) conducted a meta-analysis of 38 randomised controlled trials involving 149,051 participants and found that omega-3 supplementation was associated with reduced cardiovascular mortality, non-fatal myocardial infarction, and coronary heart disease events. DHA is concentrated in neural tissue and the retina, and observational research has linked higher circulating DHA levels with slower cognitive decline in older adults. UK dietary guidance recommends at least two portions of fish per week, including one of oily fish (approximately 450mg EPA and DHA combined), but NDNS data confirm that most adults fall short of this. A supplement providing 1,000 to 2,000mg combined EPA and DHA bridges this gap without exceeding the EFSA-assessed safe intake of up to 5g per day.
Vitamin K2 in the MK-7 (menaquinone-7) form completes the stack by addressing calcium trafficking. While vitamin D3 increases calcium absorption from the gut, K2 activates osteocalcin (which deposits calcium into bone matrix) and matrix Gla protein (which inhibits calcium accumulation in arterial walls). Van Ballegooijen et al. (2017, International Journal of Endocrinology) reviewed the synergistic interplay between vitamins D and K and concluded that combined supplementation appeared more effective than either nutrient alone for bone and cardiovascular health outcomes. Knapen et al. (2013, Osteoporosis International) demonstrated in a three-year randomised controlled trial of 244 postmenopausal women that 180 micrograms of MK-7 daily significantly decreased bone mineral density loss at the lumbar spine and femoral neck compared to placebo. A follow-up analysis from the same cohort (Knapen et al., 2015, Thrombosis and Haemostasis) found that the MK-7 group showed improved arterial elasticity while the placebo group experienced age-related arterial stiffening. At 100 micrograms daily, the dose in this stack sits below the studied therapeutic dose but above the estimated dietary intake for most UK adults, providing a proportionate baseline level.
Interaction Analysis
4 known interactions between ingredients in this stack.
Magnesium is a cofactor in Vitamin D metabolism. Research suggests adequate magnesium is necessary for the body to activate and utilise Vitamin D3 effectively.
Action: Ensuring adequate magnesium intake alongside Vitamin D3 supplementation may improve D3 utilisation.
Read full analysis →Research suggests omega-3 fatty acids and Vitamin D3 may have complementary anti-inflammatory and immune-supporting effects. The VITAL study examined their combined benefits.
Action: Taking Vitamin D3 with omega-3 (fish oil) provides the fat needed for D3 absorption. They can be taken together at a meal.
Read full analysis →Research suggests Vitamin K2 helps direct calcium mobilised by Vitamin D3 to bones rather than soft tissue, potentially reducing arterial calcification risk.
Action: These are commonly taken together with a meal containing fat, as both are fat-soluble.
Read full analysis →Research suggests magnesium may be important for Vitamin K-dependent carboxylation reactions. Both nutrients support bone health through different mechanisms.
Action: Both can be taken with a meal. No special separation needed.
Read full analysis →Suggested Timing Schedule
Morning
Fat-soluble — better absorbed with a meal containing dietary fat
Fat-soluble — take with a meal containing dietary fat
Evening
Evening preferred — may promote relaxation. Take with food to reduce GI discomfort.
Any Time
Take with a meal containing fat for best absorption. Split high doses across meals to reduce fishy burps. Freeze capsules to reduce aftertaste.
What to Avoid with This Stack
- • Vitamin K2 may interact with warfarin and other anticoagulants — consult your GP before starting
Alternatives & Variations
A daily multivitamin represents the most common alternative to a targeted stack, offering broader coverage at the cost of lower individual doses. Most multivitamins contain vitamin D3 and magnesium, but typically at amounts below the levels included here — often 400 IU of D3 and 50 to 100mg of magnesium — and rarely include meaningful quantities of omega-3 or K2. A B-complex supplement may be worth considering alongside this stack for individuals with restricted diets, particularly vegans or those over 50, where vitamin B12 absorption can decline. Probiotics address an entirely different system — the gut microbiome — and while emerging research links gut health to immune function and mood, the evidence base remains less established than for the four nutrients included here. Vitamin C is well-studied for immune support, but dietary intake from fruit and vegetables in the UK generally meets requirements for most adults, making routine supplementation less critical than correcting the documented gaps this stack targets. The rationale for a focused four-ingredient approach is straightforward: it addresses the nutrients most consistently shown to be inadequate in UK dietary surveys, at doses supported by clinical research, without the diminishing returns that come from spreading a budget across dozens of ingredients at sub-therapeutic levels.
Notes & Caveats
This stack targets the four most common nutritional gaps in UK adults. It is not a replacement for a varied diet. Individual needs differ — a blood test can identify specific deficiencies.
Customise This Stack
Load these supplements into our interactive Stack Analyzer to adjust dosages, add or remove ingredients, and get personalised timing.
Customise this stack →Frequently Asked Questions
SACN's 2016 vitamin D report set the Reference Nutrient Intake at 10 micrograms (400 IU) daily, while the NHS states that adults should not exceed 100 micrograms (4,000 IU) per day. A dose of 2,000 IU sits comfortably within this range and is widely used in clinical practice to maintain serum levels above the sufficiency threshold. Given that NDNS data show 31% of UK adults are deficient during winter months, 2,000 IU represents a reasonable dose for most adults without requiring prior blood testing. However, individuals with granulomatous conditions, kidney disease, or those taking thiazide diuretics should consult a GP before supplementing, as these conditions can alter vitamin D metabolism.
Vitamin D3 increases intestinal calcium absorption, but without adequate K2, the body has a reduced ability to direct that calcium to where it is needed. K2 activates two proteins — osteocalcin (which binds calcium into bone) and matrix Gla protein (which prevents calcium from depositing in arterial walls). Van Ballegooijen et al. (2017, International Journal of Endocrinology) reviewed evidence across animal and human studies and concluded that joint supplementation appeared more effective than either nutrient alone for bone and cardiovascular outcomes. Taking them together is a practical pairing rather than a strict biological requirement, but the complementary mechanisms make a reasonable case for co-supplementation.
In principle, yes. NHS guidance recommends at least two portions of fish per week, including one of oily fish. SACN sets a population recommendation of 450mg combined EPA and DHA per day as a weekly average. Two portions per week would approach the 1,000mg lower end of this stack's range. However, NDNS rolling programme data show that oily fish consumption across UK adults remains consistently below recommended levels. Individuals who eat two or more portions of oily fish weekly — such as salmon, mackerel, sardines, or anchovies — may not need a separate omega-3 supplement. Those who eat little or no fish, or who follow a plant-based diet, are more likely to benefit from supplementation. Algal oil provides a vegan-friendly EPA and DHA source derived from the same microalgae that fish accumulate omega-3 from.